

Low Milk Supply Stimulated by Fear
I ADORE breastfeeding! Probably my one of my very favorite things to do. I am consistently surprised by the amount of people who claim to have a lack in milk supply. When I delivered my first baby, 16 1/2 years ago, I had many friends who were breastfeeding. I honestly do not remember having regular discussion with friends who struggled with milk supply. Nor did I ever feel even concerned that I wouldn't have enough breast milk. Quite the opposite! All I knew is that's what breasts were for after you deliver......To feed your baby and produce milk. But NOW.......I have clients who quite often complain of lack of milk production OR even better have a HUGE fear that they won't have enough.
I have 2 theories on why breast milk production can be low. Of course, you have the usual issues of poor latch on or weak suck or all of the other many reasons for low milk supply. But.....I have my own opinions and beliefs as to why women struggle with milk supply. Not that the other reasons aren't valid as well but I think just considering my opinions might help a women who can't seem to get produce enough milk.
First theory......That the nutrition of the mother inherently effects milk supply. We currently live in a world where we are undernourished and over fed. Obesity is at an all time high. Even though we may look at a women who is overweight and believe that she should be able to build volumes of breast milk, studies have shown that obesity can be a factor for low milk supply. Read more about it below.


39 Weeks- Is It Long Enough To Wait?
 |
| img
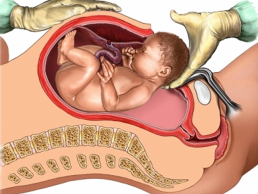
I saw this picture today and had to share! So often we feel comfortable making choices about the timing of the birth of our babies. We believe what we're being told that babies born before 39 weeks is really okay. We believe that if our babies are born before 39 weeks that they, most likely, are fully developed and all is well for their birth to come. Sad part about that last sentence is that moms are choosing to induce based solely on their personal discomfort.
Now, I know there are LOTS of reasons to induce that are truly medically indicated. Labor induction rates are about the same as c-section rates. About a 3rd of all women will use pitocin to induce labor....And just like the c-section being so high for a wide variety of absolutely ridiculous reasons.
Let me just state though that just because they are showing some of the reasons to wait until 39 weeks to deliver. I hold true that babies will come when they are GOOD and READY! Yeah, you read that right. Who knew? That babies actually KNOW when they are fully developed and it's time for them to enter the world.
So....the down low is that babies actually produce a hormone that they excrete to let the Mom know that it's time for her hormones to kick in and initiate labor. You can read all about it by clicking the link in the article below.
"Now, University of Texas Southwestern Medical Center at Dallas researchers have found that it is in fact the fetal lungs themselves which provide the signal to initiate labor.
Drs. Carole Mendelson, Jennifer Condon and Pancharatnam Jeyasuria published findings that a substance secreted by the lungs of a developing fetus contains the key signal that initiates labor." If babies really decide and know when it's time for them to be born, I'm not quite sure why we are inducing moms for labor BEFORE the initial onset of contractions has started. Waiting for baby to come when he/she is ready, limits the likelihood, like shown above, of complications with baby after birth. I believe induction is a MUCH greater risk your taking with babies ability to cope outside of the womb, than any risk that may take place by waiting until baby is ready to be born.
I've seen moms wait til 42....even 43 weeks before they delivered. GASP, you say! I foresee MUCH less risk with a mom who's babies stays in just a bit longer than a mom who wants that baby out just a bit early. A bit early has a wide variety of consequences a bit late just doesn't have. Now, there are complications that can and do take place from delivering a post date baby but the risks of induction seem far greater to me and induction is the bigger risk. You can click the link below to read more.
Patience and little understanding of the process of birth is really ALL you need to avoid an induction. But....YOU are the one the chooses how and when for your baby to be born because you LISTEN and WAIT for that baby to tell you!
In Peace,
Rachel
|
Breastfeeding ROCKS! Here's WHY!

I find it interesting that the debate of the health values of breast milk are still in full force. It seems to me that we now have enough current data that shows the increased benefits of breast milk in comparison to formula. And in my opinion, THERE IS NO COMPARISON!!
Yes, breast milk will feed your child and even somewhat nourish them. But, exclusive formula feedings can cause a WORLD of problems down the road for the health of your child. There seems to be study after study on the ill effects of formula on your baby. From common allergies to respiratory infections to ear infections. Truth be told, it may be that the actual formula is causing infections but you also are starting your child off with a compromised immune system because of the lack of needed colostrum that breasts offer.
Just so you know the numbers.....by the 1970's almost 75% of women were bottle feeding their babies. I was bottle fed and so were all the brothers and sisters. And.....when I asked other friends of mine who are around my age, if they were breast or bottle fed, almost ALL of them were bottle fed.
Click the link below and read about it for yourself. I'm just shocked at our ignorance on the subject and, it seems, so many women's and couples refusal to learn more about breastfeeding and why it's REALLY best!
I understand that there are those rare and few women who cannot breastfeed their babies because of lack of breast milk production or other reasons. But....as a women who has lost ALL of her breast milk before and regained it back within a month AND who has breast fed ALL 5 of my children for over a year, ( my last I nursed until she was 3 1/2 or so), AND who has helped MANY, MANY other women learn how to breast feed their own children........I believe it is very RARE to not be able to breast feed your baby. (If you want to know more about this or are curious to find out how you can make that happen EVEN when you haven't been able to in the past, feel free to email me)
Formula can literally change the gut flora of the intestinal tract with just one bottle. Our intestinal tracts has millions of little microflora or good bacteria that feed almost EVERY physiological function of the body. When that AMAZING microflora is damaged in any way, it then sets the stage for each system of the body to start a potential break down process in the health of the person. That break down process can take YEARS to manifest itself. It doesn't have to happen over night. Click the link below to understand more about how formula can potentially forever change the health of your child.
- "Infant formula should not be given to a breastfed baby before gut closure occurs.
* Once dietary supplementation begins, the bacterial profile of breastfed infants resembles that of formula-fed infants in which bifidobacteria are no longer dominant and the development of obligate anaerobic bacterial populations occurs. (Mackie, Sghir, Gaskins, 1999)* Relatively small amounts of formula supplementation of breastfed infants (one supplement per 24 hours) will result in shifts from a breastfed to a formula-fed gut flora pattern. (Bullen, Tearle, Stewart, 1977)* The introduction of solid food to the breastfed infant causes a major perturbation in the gut ecosystem, with a rapid rise in the number of enterobacteria and enterococci, followed by a progressive colonization by bacteroides, clostridia, and anaerobic streptococci. (Stark & Lee, 1982)* With the introduction of supplementary formula, the gut flora in a breastfed baby becomes almost indistinguishable from normal adult flora within 24 hours. (Gerstley, Howell, Nagel, 1932)* If breast milk were again given exclusively, it would take 2-4 weeks for the intestinal environment to return again to a state favoring the grampositive flora. (Brown & Bosworth, 1922; Gerstley, Howell, Nagel, 1932)"
If you haven't read WIKIPEDIA and what they say about the breastfeeding.....YOU SHOULD! They have quite a bit of information of all kinds on the subject of breastfeeding. Good stuff!!
Since we are on the breast feeding topic and since I breastfed my daughter for over 3 years, I thought I would share this video. Our perspectives on breast feeding have been SEVERELY skewed, in my opinion. All around the world, length of breastfeeding rates vary. As Americans, we tend we wean our children MUCH earlier than other countries do. I often wonder why that is? Here's a video on women who breast feed older children in public and some of the reactions they were getting for doing so.
And lastly, a FUNNY little article I saw today that I HAD to share because I think this women is HILARIOUS!! Enjoy!
Click on the link below to read the article.
Please educate yourself on ALL the advantages for both you and baby for breast feeding and DO YOUR BEST to make sure you give your newborn the beginning he/she deserves!
In Peace,
Rachel

Reminder: Kale Chip Class TOMORROW NIGHT! Read Below
Just a reminder about tomorrow's class!! Here's some preview pictures of the kale chips I've been making! This will be a FUN class.....Don't miss it! Hugs, Rachel



- How to make 2 different flavors of kale chips- MY cheesy kale chips (of course) & a SURPRISE flavor!
- The benefits of raw foods and why more raw foods creates increased health and happiness in your LIFE!
- Find out why kale is one of the BEST foods for you!
- Learn the health benefits of ALL the other ingredients put into the kale chips
- Understand more about how your body responds to the AMAZING health benefits of kale chips
- See the ease of making kale chips and learn how to incorporate them into your life
- Of course.....you will be tasting and trying each of the kale chips
- Lastly, I will have extras to SELL at the end of the class

Love & Nurturing Stimulates Larger Brains In Our Children
This isn't a surprise, really? I mean....is it? I only ask the question because it seems to make logical sense to me that when we nurture and love our children, the WAY they were meant to be loved and nurtured.....then, of course, they'd be more intelligent and grasp new ideas about the world around us in a healthier way! I believe that LOVE is truly the only healer and worker of magic when it comes to total health and happiness. How can it not stimulate our children's brains to grow larger so as to hold more information and build a greater curiosity of the world around them?

I wonder if the brain growth and size takes place because growth, of any kind, can be stymied by fear. If a child enters the world feeling a sense of dread and fear of the world around them....I wonder....do their brains then restrict growth to be able to protect the infant of exploring too far the world around them? If they can't comprehend more, then maybe the system believes they can protect themselves from treading too far into a scary, unsafe world? I have no factual evidence to correlate with my opinion & honestly, I'm too lazy to spend the time looking....but what if????

Birth itself can be extremely traumatic on a newborn. Their nervous systems are about 150 times more sensitive than ours as adults. That only means that their ability to view their own birth experience as traumatic is much greater. Looking into the world of how we birth our children.....not just their treatment and care after delivery, might feed into the insights and studies that are being done on children's brains.
I have no doubt that growth restrictions can even take place in utero. This can happen based upon the Mother's fears and negative belief patterns about herself or the world at large. She then passes those fears and negative belief patterns onto her unborn child in an attempt to help the baby acclimate to the new world it's entering. It's a protection, you see. The only downfall with that protection is then the baby inability to feel safe in our world and choose to explore it. Exploration and experience truly are the greatest teachers for our children.
Below is the first article which shows an image of 2 brains. One where the child was nurtured and love and the other where the child was extremely neglected. Notice that the neglected infant's brain is almost half the size of the loved child. This is a HUGE difference! Not just a mild one......Click the link below to read the full article.
"Experts say that the sizeable difference in the two brains is primarily caused by the difference in the way each child was treated by their mothers."
The article states that not only will the child's brain size be smaller but that there are also LONG term effects of the restricted growth.
The first hour or so following birth can be some of the MOST CRITICAL bonding and connecting time for you and your baby. Think back about the birth of your own children. Did they whisk your baby away immediately after birth or did they let you hold and cuddle your baby for as long as you wanted? Did they poke and prod your baby with needles and hands or did they keep your baby close to you as they gently talked and soothed your baby as they did any needed testing? These are just 2 examples of a stressful situation for you and your baby that might negatively effect your baby's ability to feel love and their brain growth patterns.
This second article is explains more in details the REASONS for the restricted brain growth and why and how it happens. Here's a great quote from it.....
"Myths inevitably survive long after they’ve been scientifically disproven. Such is the case with the fantasy that mental illnesses can be written off solely to genes and chemicals. Over the last decade a string of scientific discoveries has shown that the biology driving mental illness has at least as much to do with the environment as with chemicals or genetic inheritance. And it increasingly appears that the single most powerful environmental factor is the love - or its lack - that children receive from their parents. So in a very real way we parents are back on the hook for the lifelong emotional well-being of our kids."
Click link below to read the whole article....
Know the Signs & Ways to Avoid a C-Section
 |
| img |
So....I have passionate feelings about our current c-section rate which seems to be holding strong at 32%. We all know what 32% means, right? Let me spell it out a little bit more.....32% means that 1/3 of ALL babies in the United States are getting surgically cut out of Mom's. That's one in every 3 women. Does that seem extreme to you? Because it, MOST DEFINITELY, does to me.
Did you know that in some areas of the United States the c-section rate can be as high as 50-60%? This seems ABSOLUTELY ridiculous to me but Brazil actually carries a 82% c-section rate.....82%!!!! Can you believe it? I read that number and honestly, my head just spins.
The most fearful part about that 82% is that we, as American's, are on the same road. I am aghast that women will blindly walk into the operating room and say NOTHING! Or even worse, request that their baby is surgically removed. Please don't get me wrong, I believe in every woman's right to choose whatever birth experience she wants but.....I believe that choice should only be made after proper experience, understanding and knowledge of what a c-section is and the consequences to choosing to have one.
Read more about that 82% c-section rate at "BRAZIL WOMAN REBEL AGAINST C-SECTIONS"
 |
| img |
Below is some information from Wikipedia about what The World Health Organization believes are c-section rate should be. They feel it should be cut in half at 15%. I recommend searching this subject online to get more information about it but some studies have concluded that, in the United States, our c-section rate should be as low as 10%.
Analyzing the rise in Caesarean section rates
The World Health Organization has determined an “ideal rate” of all cesarean deliveries (such as 15 percent) for a population. One surgeon's opinion is that there is no consistency in this ideal rate, and artificial declarations of an ideal rate should be discouraged. Goals for achieving an optimal cesarean delivery rate should be based on maximizing the best possible maternal and neonatal outcomes, taking into account available medical and health resources and maternal preferences. This opinion is based on the idea that if left unchallenged, optimal cesarean delivery rates will vary over time and across different populations according to individual and societal circumstances.[65]
The question is.....why are c-section rates so HIGH? Well, of course I believe their are a variety of reasons. Those reasons go anywhere from a busy doctor feeling more in control of the birth environment by performing a c-section so he recommends them regularly to a intervention overload which baby cannot handle and the inevitable response is baby struggling during delivery.

But.....in my opinion (which doesn't matter much really), the reason for the HIGH c-section rates really is just lack of education on the part of the mother and the father. I gotta be honest, I'm always a bit surprised when I meet a couple who is getting ready to deliver their first baby and their understanding of the birth process is almost non existent.
Now, the mother in her wisdom, will hopefully make wise choices in her care provider while educating herself on the process of conception, pregnancy and birth. This is her BEST BET to A) avoiding a c-section and B) create and stimulate a BLISSFUL pregnancy and birth for herself. With all that being said, below are some interesting link I recommend you click on to educate yourself and be more aware of your choices and how to avoid a c-section.
I truly believe that education is KEY to knowing, finding, creating and having an AMAZING pregnancy and birth. It just is! We may have LOTS of other answers to fixing the problem. And I'm sure they are VERY good answers. But....education lifts the wisdom of a women to a place where she finds her power and strength to deliver her child in peace and joy.
First: Here is an EXCELLENT article that should help you understand the "set-up" for the c-section. Click on the link below.
"TOP TEN SIGNS YOUR DOCTOR IS PLANNING TO PERFORM AN UNNECESSARY CESAREAN SECTION ON YOU"
Second: Here are 2 great article showing you how you can avoid a c-section and what actions you might take. Click on the links below!
"TIPS AND TOOLS FOR AVOIDING A CESAREAN SECTION" -The Childbirth Connection is a very informative website and I would take the time to search their whole site. :)
"5 WAYS TO AVOID A C-SECTION"- As you read this article, educate yourself on what it means to have a "medically necessary" c-section. So often we confuse the opinions of our doctors with what a true medical emergency is. Find out BEFORE you deliver and then when your doctor throws out big words as to why you need a c-section, your decision will be based in your knowledge and not fear of the situation.
Lastly: It only makes sense that the Amish might have answers to help lower the c-section rate. But....the answer almost always is.....if you want to avoid a c-section....The MORE you leave a mother ALONE during her birth process, the MORE likely her birth will be a safe, vaginal birth. Click the link below to find out what's working for the Amish.
"AMISH OFFERS CLUES TO LOWERING US C-SECTION RATES"
Have a VERY happy Wednesday!
In Peace,
Rachel
P.S. I didn't even go into the potential birth trauma for Mom and baby during and after a c-section. Check back for another day where I will touch on that subject. But again....another point to look at when educating yourself about c-sections!
Raw Kale Chips Class~ Jan. 29th @ 7 pm
I'm so EXCITED to teach how to make raw kale chips! Please pass this info along if you know others who might be interested.....:)

- How to make 2 different flavors of kale chips- MY cheesy kale chips (of course) & a SURPRISE flavor!
- The benefits of raw foods and why more raw foods creates increased health and happiness in your LIFE!
- Find out why kale is one of the BEST foods for you!
- Learn the health benefits of ALL the other ingredients put into the kale chips
- Understand more about how your body responds to the AMAZING health benefits of kale chips
- See the ease of making kale chips and learn how to incorporate them into your life
- Of course.....you will be tasting and trying each of the kale chips
- Lastly, I will have extras to SELL at the end of the class
Fatness Is Predisposed In Utero
So just another article that delves into the world of pregnancy and nutrition, my 2 LOVES! I'm excited to think we are striving harder through more research to find out what is really taking place in the womb and what effects nutrition plays to the unborn fetus.
Of course, I can only speak from my experience, but nutrition played a huge roll in my overall conception/pregnancy/labor/birth/postpartum experience. You can read more about my experiences in my pregnancy in my post, "FAT IS NOT WHERE ITS AT-MEDICATING OUR UNBORN BABIES FOR OBESITY."
I do feel quite passionate about health BEFORE pregnancy and consistent high nutrient dense foods during pregnancy and beyond. As stated in the article below, your baby could be predisposed for diabetes, a disease that is actually quite simple to heal.
This quote from the article below is extremely bothersome for me.....
There is an EXCELLENT documentary called "SIMPLY RAW: REVERSING DIABETES IN 30 DAYS." You read that right.....curing diabetes in 30 days. It actually happens, folks. But think about it, what if we could STOP completely your baby from ever showing signs of diabetes. Imagine if illness, in general, could totally be thwarted for your unborn child.
Well, it just so happens that I live in a world where I believe that is a reality. I actually believe you can CURE ANYTHING. Dr. Christopher truly said it best...."There is no such thing as an incurable disease, only incurable people." I wholeheartedly agree with this quote. He is RIGHT ON.
Before pregnancy, your health is completely up to you! During pregnancy, your health and the health of your unborn child are BOTH up to you! I think there must be some kind of disconnect in our world that pregnant women don't seem to be understanding this concept. Please know I make that remark not out of judgement because I have been one of those disconnected women. But rather I say it out of concern and fear for our future generations health and well being.
At some point, in order for our world to be a healthier and happier place, women will have to really take FULL responsibility for themselves. They will have educate themselves on foods, herbs and nutrition in general to know what is REALLY best for you and your unborn child.
Honestly, that education takes time. It takes planning and preparation BEFORE conception to really make that happen. I am always in AWE of the couples who attend my LivingMom Childbirth Educational Courses BEFORE they conceive. As I've watched them during their pregnancies, they are healthier and happier than I believe they would of been without that education and understanding. Of course, this is all my opinion but I have closely watched these women and it makes a PHENOMENAL difference later on. It just does.
Yet again, I'm stepping down from my soap box. I believe our bodies and the bodies of our growing infants deserves the BEST quality foods to keep it running at peak performance. My hope is that women will go the extra mile to do their very BEST for themselves and their babies. I believe the majority of women already do so and its merely the lack of education that prevents the ideal pregnancy/birth experience. It just takes that first step to make a lasting change.
In Peace,
Rachel
_________________________________________________________________
Children’s Body Fatness Linked to Decisions Made in the Womb
Boob Jobs & Longer Labors Than 50 Years Ago
I know all of you have missed me and my AMAZING blog posts. Just kidding....:) Well, I'm back. I took so long off because I decided to have surgery. Can you believe it? Yes, healthy living....crunchy mama....ME..... decided it was time to fix a surgical hernia, have a scar revision.....AND while we're already cutting me open.....get a BOOB JOB! You read that right....YES, I am one week out from a breast augmentation and lift.
Now, I'll be honest, I am a woman who prides herself on being tough. Growing up, I was a phenomenal baby in almost every way. I avoided anything that might show the remotest sign of being in any way painful at all costs.
I still remember when I told my family we decided to have a home birth. I can still hear the constant laughter ringing in my ears. My family actually thought I was joking at first. They regularly commented that there was NO WAY I was going to be able to do it. That I couldn't handle pain like that without whining and crying every step of the way.
Well, since that time I have had 5 babies at home, 3 abdominal bowel surgeries, regular bowel obstructions for 4 years straight (that in my opinion hurt just as much if not more than having a child) and the hernia repair, scar revision and boob job.....have TOPPED them all. I came home and for the first 4 days thought...."What the HELL have I done."
Today is the ONE week mark since the surgery. I'm priding myself today on the fact that I actually took a shower. I even shaved my legs. This is a BIG deal, people! Just 3 days ago I was still wallowing in the fact that I'd made a HORRIBLE mistake and recovering from boob job surgery is literally choosing to live in hell for about 5 days.
So I guess the jury is still out.....Am I a total WIMP or is major surgery a HUMONGOUS PAIN? I'm speaking both literally and philosophically here. :) I am on the UP and UP! I actually took a shower today which is a BIG feat in and of itself for me. I do feel a little like WONDER WOMAN! Yes, I'm learning to deeply LOVE myself even in the lies I tell myself. LOL!!!
So, since every post has to have some WONDERFULNESS about babies and mamas and birth, I've decided to post the article below. It is disheartening to think that labor now takes longer than it used too.
My opinion.....LEAVE moms and babies and Dads....ALONE during the birth process, labor will be shorter and quicker and LESS painful....IF even painful at all. Its that SIMPLE!!! Let nature and nurture do their jobs and low and behold, relaxation and serenity step in to create a birth that feels easy and blissful and usually ends up happening quite FAST!
Have a Terrific Thursday!
In Peace,
Rachel
__________________________________________________________
Babies Take Longer To Come Out Than They Did In Grandma's Day

Your Children Are Part Of You FOREVER!
I had to share this today. It made me cry. I love my children in EVERY way possible and this article brought up some WONDERFUL emotions. My oldest turns 16 tomorrow. I can't believe how quickly the time has flown. I didn't ever realize the rush of time that would pass without my even recognizing it.

As I think back on my pregnancy, labor, birth and life thereafter with Dean, I've been saddened as he becomes a teenager and a man. To watch your children grow up with the eventual goal of leaving your home to form their own families, is both heart breaking and exciting at the same time.
I've shed many, many tears as I watch Dean become who he REALLY is and find himself. Though, at times, its painful and overwhelming, I know his personal growth will only aid in him delightful new ways.
While reading this article and watching the video below, I realized, yet again, that my babies will really never leave it. That because they were created from my egg and were grown in my belly, they would be part of me forever. Its so exhilarating to have science now prove that our children's cells are actually forever in our bodies. Especially in our hearts.....
I LOVE the world of science and what it is now proving. So many things we used to believe were just weird, strange ideas and philosophies, science is now proving is actually a REALITY!
When I ponder the loss I might feel in watching my children grow up, I will stay focused on the parts of themselves I gave them and they gave me. That we will ALWAYS be connected and NEVER apart!
I hope all mothers out there will do the same.
In Peace,
Rachel
__________________________________________________
Why Babies Should Never Sleep Alone
I did just recently put a post together called "Co-Sleeping: The Facts And The Benefits." But because I absolutely ADORE co-sleeping in EVERY way, I had to post the article below. I wholly agree with this article and its ability to define even more acutely how co-sleeping IS safe. Its when we don't understand how to keep it safe, that we then see problems.
Co-sleeping with my kids brought such JOY for us. Chris and I were in AWE each time we had the opportunity to share the bed with our new little tiny one. I do agree that there are biological process involved that make co-sleeping so enjoyable.
I let you have at it and decide for yourself what you think. Truthfully, the fact that I could SLEEP the WHOLE night even while breastfeeding was the deciding factor for me. It just makes your world that much brighter....:)
In Peace,
Rachel
P.S. Below is a fun little video Chris took a few months ago trying to wake our kids up. Our kids, because of co-sleeping, LOVE to all sleep in the same room together sometimes. So Mabel, Millie, and Pratt made a bed on Golden's floor so they could all be in the same room. For the longest time, all 5 of our kids slept in the same room together. They really, really LOVE each other. Its is WONDERFULLY adorable. :) And yes, This is how long it takes to wake our kids up....
_______________________________________________________
Cosleeping and Biological Imperatives: Why Human Babies Do Not and Should Not Sleep Alone
 By James J. McKenna Ph.D.
By James J. McKenna Ph.D. I am not alone in thinking this way. The Academy of Breast Feeding Medicine, the USA Breast Feeding Committee, the Breast Feeding section of the American Academy of Pediatrics, La Leche League International, UNICEF and WHO are all prestigious organizations who support bedsharing and which use the best and latest scientific information on what makes mothers and babies safe and healthy. Clearly, there is no scientific consensus.
I am not alone in thinking this way. The Academy of Breast Feeding Medicine, the USA Breast Feeding Committee, the Breast Feeding section of the American Academy of Pediatrics, La Leche League International, UNICEF and WHO are all prestigious organizations who support bedsharing and which use the best and latest scientific information on what makes mothers and babies safe and healthy. Clearly, there is no scientific consensus.World's First GM Babies: Really? What's Next?
Um....the article below is SERIOUSLY disturbing. I think this is subject matter that should be discussed in the world of epigenetics. I just read the article this morning and I'm still in a bit of shock. This is truly the beginning of potential drastic change in the human species. We are entering a world where we are no longer utilizing the gifts of natural selection but taking control over nature.
Notice the blue strawberry below. Look at it closely....does it look or feel natural to you ? I just reposted this on Facebook and had a few comments about it tasting delicious. Honestly, I just really don't care how good it is or isn't. The fact that it is cross bred with a Arctic Flounder Fish. It just sounds WRONG! Maybe its just me....
I have yet to believe that ANYTHING we create in regards to ANY modern technology would be greater or better than what the Divine or Grand God/Goddess can create. I feel afraid at the outcome of these changes to our society as a whole and the individual. I see something with this large a change in human kind should have YEARS worth of studies. I don't even know what else to say at the moment. Feel free to share your comments or opinions in the bottom.
In Peace,
Rachel
 |
| Scientists have come up with a Blue Strawberry by splicing them with Fish genes: Scientists are genetically modifying strawberries in order to allow them to resist freezing temperatures better. They're doing it by artificial transfer of genes from a species of fish called the Arctic Flounder Fish. The Arctic Flounder Fish produces an anti-freeze that allows it to protect himself in freezing waters. They isolated the gene that produces this anti-freeze and introduced it to the strawberry. The result is a strawberry that looks blue and doesn't turn to mush or degrade after being placed in the freezer. While they're not in production, research is ongoing. |
_________________________________________________________
___________________________________________________________
World's first GM babies born
Epigentics: The Environment Defines The Imprinting
The article below is fascinating! Again, more evidence that our DNA patterns can and DO shift based upon the inner uterine environment. The idea that all our sensory experiences, thought patterns and experience are encoded in the DNA and that DNA can and does change and shift is hard for some people to digest. As science works its magic, its proving this theory to be absolutely TRUE!
 |
| img |
Differences Between Human Twins at Birth Highlight Importance of Intrauterine Environment
Stepping Outside The Birth Box

I recently heard the song below and was fascinated by it. It was written in the 60's, a time of feminism and personal exploration. A HUGE awakening was taking place where people found a new way of thinking and being. I believe we are making a similar transition NOW in our world. Especially when it comes to BIRTH!
We are in a birth revolution and its VERY EXCITING! Women, men and families are taking back their rights to birth how, when and where they choose. They are standing up for freedom in pregnancy and birth and doing what they can to stimulate change and education. Its AWESOME and INSPIRING in every way.
Sixteen years ago, I noticed a small and subtle shift taking place. At that point, I still talked with women who thought I was COMPLETELY crazy (which I am, btw, I'm not afraid to admit it) that I chose homebirth and waterbirth and even just plain 'ol natural childbirth. Just choosing to have your baby without any drugs was a concept most women scoffed at.
It was been a wonderful ride to see the courage, strength and personal empowerment of women and men to speak UP about the abuses and violence that currently take place in birth. The level of control and falsely held beliefs surrounding birth seemed to stymie any growth for change within the birth environment for years. That is NO LONGER!
My experience has taught me that since the invent of the computer and the easy access to information has made, we've seen the BIGGEST differences. Education is the key that opens the door to understanding and removal of myths and fears revolving around birth. I know that sounds so simple but it really is.
I watch the faces of those who attend my childbirth classes and see a sense of bewilderment at where we are as a society and nation when it comes to birth. They feel lost. They feel scared. Once they learn the truth about birth, the inherent safety of it when left alone, and the intelligent capacity of their bodies to birth healthy babies, I see a couple who can move forward making positive birth choices based on truth, understanding and trust of human kind. Its truly enlightening to watch!
I hope you enjoy the video below. Its time to rip ourselves outside of the "birth box" and open new avenues for confident change in birth. It really is time to unbind a women's hands and offer her freedom in her birth choices. Its time to be, as Malvina Reynolds herself is, A REVOLUTIONARY!
In Peace,
Rachel
Props For All The Midwives
Excellent video on the benefits of midwives! Its unfortunate where we are nation wide when it comes to midwifery care and home birth. Things seem to be looking up and changing....but very slowly!